By Keisuke Fujita, M.D., Ph.D.; Hidehiko Beppu, Ph.D.; Kaoru Kawai, Ph.D. & Kan Shinpo, Ph.D.
Institute of Pharmacognosy, School of Medicine, Fujita Health University – 1992
Originating along the Mediterranean coast, Aloe (Aloe arborescens Mill var. natalensis Berger) has served mankind through the ages, preventing disease in Alexander the Great’s soldiers during military expeditions, curing the obstinate eczema of Chinese Tang dynasty poet, Liu Yu Xi, and treating some latter-day ills like gastric ulcers, cancer, as well as burns.
In ancient Greece Aristotle taught Alexander the Great about the efficacy of Aloe. The hero gave it to his soldiers to maintain their health on campaigns.
Liu Yu Xi recorded his experience with Aloe or “rokai” as it was known in Chinese medicine: “When I was a child, I suffered from obstinate eczema. I used various medicines, but they were ineffective. However, when I used Aloe, which a drug merchant recommended me, the eczema healed rapidly.”
Our team recently assessed the effects of Aloe scientifically, using modern medical methods, and recorded its findings of Aloe’s effects as an anti-inflammatory agent, gastric ulcer suppressant, blood glucose normalizer, anti-cancer treatment and Aloe’s anti-inflammatory suppressant action on burn and injury aggravation.
The most common use of Aloe is to apply it to cuts and burns. Some readers may recall their grandmother picking Aloe, growing along the veranda, and applying its juice to a cut or burn, and feeling the rapid relief of pain.
In vitro demonstrations show that extracts from Aloe degrade bradykinin, a substance responsible for pain and inflammation after injury. Carboxypeptidase is the active ingredient of Aloe which produces the anti-inflammatory action.
Burns are known to progress along the following course: pain, redness and fever, edema, necrosis and dysfunction. Aloe suppressed the burn’s aggravation by suppressing the pain and edema.
Aloe is effective not only when applied topically, but also when taken orally. Oral treatment is more effective because it acts on the affected tissue via blood vessels.
Figure 1 shows the effect of oral Aloe treatment on rats with experimentally induced foot burns. The rats were divided into three groups: Group A (rats without oral Aloe treatment) and Groups B and C (rats orally treated with Aloe). The size of edema was smaller in Groups B and C than in Group A. If grandmother had said “chew on this piece of Aloe,” your wound would have healed more rapidly than with a topical application.
Figure 1
Suppression of edema
The size of edema is larger in Group A (without oral Aloe treatment) than in Groups B and C (orally treated with
Aloe).
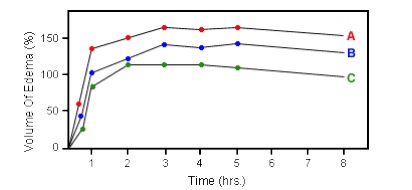
Group A: no oral Aloe treatment
Group B: oral treatment with Aloe extracts rich in ingredients of moderate molecular weights (10,000 to 50,000)
Group C: oral treatment with Aloe extracts rich in ingredients of higher molecular weights (over 50,000)
Effect on Gastric Ulcers
Aloe is also known to favorably affect the stomach and intestinal track. Gastric ulcers are a very common disease in our modern stress filled world. Aloe, which suppresses gastric ulcers, can be regarded as a household medicine for people who suffer from this disease.
Simply speaking, gastric ulcers are a condition where one’s own gastric juice has digested the stomach. Gastric juice, primarily containing pepsin, is secreted from the stomach to digest food. Normally, gastric juice does not digest the stomach because of a protective layer of superficial membrane composed of neutral mucous cells shielding the gastric wall.
However, once a hole is created in this membrane due to stress or other causes, the pepsin digests the gastric wall resulting in ulceration.
Aloe first suppresses the action of pepsin itself, and then, a polysaccharide contained in Aloe promotes the repair of the protective membrane.
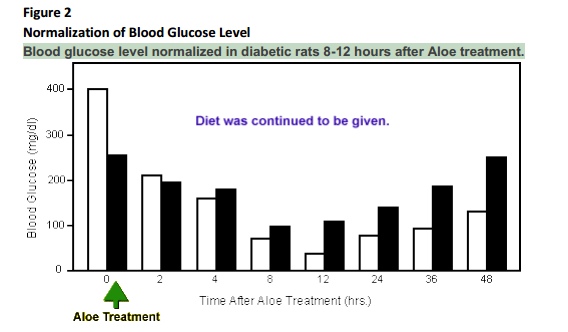
Reduction of Blood Glucose in Obese Middle-Aged Diabetics
At the present time, people tend to eat excessively and get little exercise, factors that can be attributed to an increasing prevalence of diabetes mellitus. Aloe has been shown to be a highly effective treatment for diabetes.
There are two of diabetes mellitus: insulin-dependent diabetes mellitus (IDDM) and non-insulin-dependent diabetes mellitus (NIDDM).
In patients with IDDM, insulin is deficient, requiring daily insulin injection. On the other hand, NIDDM can be controlled with diet therapy without requiring insulin injections.
Obesity triggers NIDDM among people in age groups susceptible to adult diseases. Some strains of mice used to test Aloe’s effect also developed NIDDM in the presence of obesity. We examined two such strains.
Figure 2 shows that in both strains of mice, Aloe injection reduced blood glucose level to a normal range (120 mg/dl) 8-12 hours after injection.
Additional studies focusing on testing Aloe’s effects on IDDM induced mice.
Insulin is secreted from the beta cells of the islet of the pancreas. Treatment with streptozotocin (Sz) is known to destroy the beta cells causing diabetes mellitus. We experimentally induced IDDM in mice by Sz treatment, and then administered Aloe.
In this experiment, Aloe was given in two forms: Aloe A (superficial green-colored portion of Aloe leaf) and Aloe B (the inner white-colored fleshy portion of Aloe leaf). Both Aloe A and Aloe B reduced blood glucose level to a normal range.